Introduction: The Sci-Fi Dream Meets 2026 Reality
If you’re looking for the moment the hype finally became reality, look no further than the clinical landscape of 2026. A decade ago, the idea of editing human DNA to cure disease was the domain of late-night science fiction and speculative laboratory papers. Today, it has matured into a formidable medical platform with approved therapies and active human trials.
But while the molecular “scissors” are sharper than ever, the target—cancer—is proving to be a stubborn adversary. We are seeing headlines promising that gene editing will imminently replace chemotherapy or that a universal “one-shot” cure is around the corner. The biological reality, however, is far more nuanced. Before we can appreciate where we’re going, we need to understand the tool itself. CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats) is a technology that allows scientists to cut DNA, remove specific genetic sequences, and insert new ones to modify cellular behavior. By using the Cas9 protein as “molecular scissors,” researchers can now reprogram cells with a level of precision that was once unthinkable.
The Milestone: CRISPR is No Longer Theoretical
The transition of CRISPR from a theoretical platform to a validated medical technology reached its most significant turning point with the approval of Casgevy. Developed by Vertex Pharmaceuticals and CRISPR Therapeutics, Casgevy is the first CRISPR-based therapy to move from the lab to the pharmacy. Designed to treat blood disorders like sickle cell disease and beta thalassemia, its approval was a historic victory for safety validation.
For the medical world, Casgevy provided the essential “proof of concept.” It demonstrated that gene editing can be performed safely and effectively in human patients without catastrophic side effects. This success in blood disorders is the bridge the oncology world needed. If we can successfully edit a patient’s blood cells to treat a chronic disease, the logical next step is applying those same “scissors” to the cells involved in cancer.
The Biological Wall: Why Cancer is the “Final Boss” of Gene Editing
Treating a blood disorder like sickle cell is often a matter of fixing one clear, localized genetic target. Cancer, by contrast, is the “final boss” of genetics. It is not a singular target; it is a moving one. The primary reasons cancer is so difficult to “edit” out of existence include:
- Genetic Messiness: Unlike blood disorders, cancer usually involves dozens or even hundreds of mutations.
- Internal Diversity: Even within a single patient, tumor cells are heterogeneous—meaning some cells may respond to an edit while others remain untouched.
- Constant Evolution: Tumors are biologically adaptive, evolving rapidly to survive the body’s defenses and medical interventions.
- Hard-to-Reach Targets: While blood cancers are easier to access, “solid” tumors like those found in the brain, pancreas, or metastatic sites remain shielded by complex biological barriers.
“Cancer is not one disease. It’s thousands of biological problems.”
The Reality Check: Off-Targets and Price Tags
As we move toward 2035, two major hurdles remain: safety and cost. Regulators remain cautious about off-target edits, where CRISPR occasionally cuts unintended regions of DNA. These accidental edits can lead to unwanted mutations or long-term complications that may not appear for years.
Furthermore, the economic reality is staggering. Current advanced gene therapies can cost anywhere from hundreds of thousands to several million dollars per patient. For CRISPR to become a mainstream oncology tool rather than a luxury for the few, the industry must solve the massive challenge of cheaper manufacturing and automated delivery.
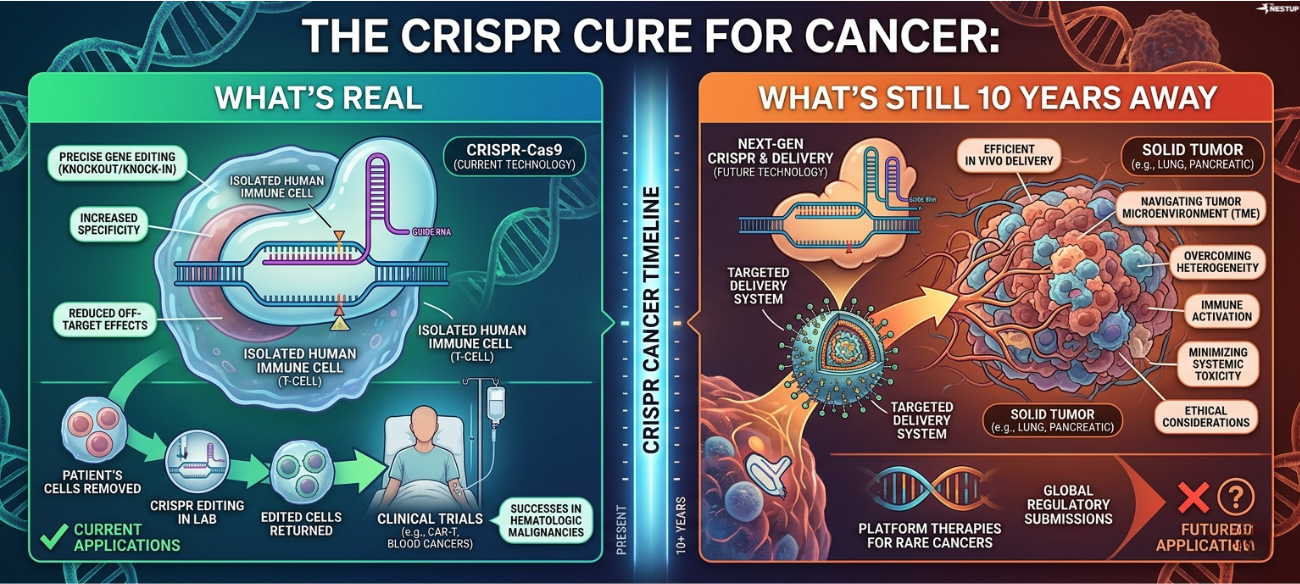
The Current Strategy: We Aren’t Editing Tumors—We’re Editing the Body’s Defense
In 2026, the most effective strategy isn’t trying to “fix” the messy, mutating DNA of a tumor directly. Instead, we are editing the patient’s immune system to be a better hunter. This is the era of CRISPR-enhanced CAR-T Therapy.
In this process, doctors remove a patient’s T-cells and genetically modify them in a laboratory using CRISPR. These modified cells are then infused back into the patient, where they act as a biological search-and-destroy team.
One major advantage of this approach is enhanced targeting. By using CRISPR to “knock out” certain genes, scientists can program T-cells to recognize cancer markers more accurately and ignore the signals tumors use to “hide” from the immune system.
Additionally, this method offers a significant reduction in relapse risk. Because the edited immune cells stay in the body, they provide a durable, living defense that can prevent the cancer from returning. Finally, the move toward “off-the-shelf” therapies is accelerating, with the goal of creating standardized, pre-edited immune cells that don’t need to be custom-made for every individual patient, potentially lowering costs and wait times.
The Delivery Bottleneck: The Struggle of In-Vivo Editing
Currently, most success stories are Ex-vivo (lab-based) edits, where cells are removed, edited, and returned. The “holy grail” of biotech is In-vivo editing—performing the surgery directly inside the patient’s body. This would allow us to treat cancers that are currently impossible to reach with traditional surgery.
The bottleneck isn’t the “scissors”—it’s the “delivery truck.” Getting the CRISPR machinery to the right cells at the right dose without harming healthy tissue is the hardest unsolved problem in the field. Current delivery methods include:
- Lipid Nanoparticles: Tiny fat bubbles that carry the genetic code.
- Viral Vectors: Re-engineered viruses that “infect” target cells with the edit.
- Engineered Delivery Proteins: Specialized proteins designed to act as a homing beacon for specific cell types.
“Delivery may matter even more than editing accuracy.”
The AI Catalyst: Designing the Future of DNA
If CRISPR is the tool, Artificial Intelligence is the architect. In 2026, AI is the primary engine accelerating drug discovery. The synergy between these two technologies is shortening research timelines from decades to years.
AI is currently performing four critical roles:
- Designing CRISPR Guides: These guides act as the “GPS” for the molecular scissors, ensuring they find the exact DNA coordinate.
- Predicting Protein Structures: Helping scientists visualize how an edited cell will behave before it is even created.
- Optimizing Delivery: Using algorithms to design the most efficient lipid nanoparticles to penetrate tumors.
- Target Identification: Sifting through mountains of genetic data to find new vulnerabilities in hard-to-treat cancers like pancreatic and brain tumors.
A Realistic Timeline: Managing the 10-Year Hype
While we are not yet at the stage of a “universal cure,” the roadmap for the next decade is clear.
| Timeline | Likely Progress |
| 2026–2028 | Expansion of CRISPR trials for various blood cancers and simpler genetic targets. |
| 2028–2032 | Improved attempts at In-vivo editing for localized, accessible targets. |
| 2030+ | Growth of scalable, personalized oncology therapies as manufacturing costs drop. |
| Beyond 2035 | Potential for broader, reliable applications in complex, metastatic solid tumors. |
Conclusion: The Shift Toward Programmable Medicine
The bottom line in 2026 is that CRISPR has successfully entered the clinic, but it has not yet conquered cancer. We are witnessing a fundamental shift in the philosophy of medicine: we are moving away from traditional “chemical” treatments like chemotherapy and toward an era of programmable cellular engineering.
The future of health is increasingly viewed through the lens of biological code. Now that we have the tools to program our own cells, we must face the next set of challenges: Are we prepared for the economic hurdles and the biological complexities that come with “re-coding” human health? The tools are ready; our ability to deliver and afford them will define the next decade of medicine.
")
{kind=link}